The Practice of Catheter Cryoablation for Cardiac Arrhythmias
Edited by Ngai-Yin Chan


Cases
Case 4.2. Catheter cryoablation for Atrioventricular Nodal Reentrant Tachycardia (AVNRT)
A 61-year-old man with a history of hypertension and obstructive sleep apnea presented with recurrent paroxysmal palpitations, despite treatment with verapamil. An electrocardiogram (ECG) during palpitations revealed supraventricular tachycardia (SVT) (Figure 1A). ECG during sinus rhythm is shown in. (Figure 1B See also Video Clip 4.1.)
Cardiac electrophysiology was performed and revealed dual atrioventricular (AV) nodal physiology with inducible single AV nodal echo beat. No AVNRT was inducible.
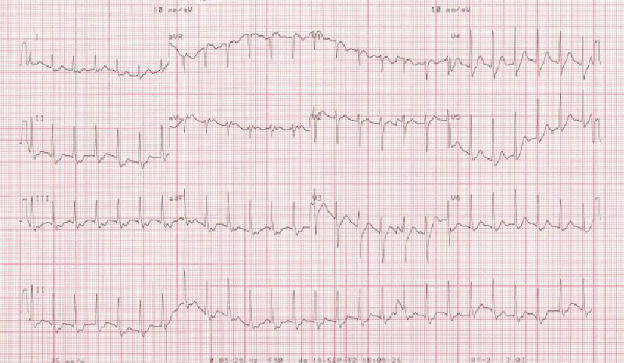
Figure 1A
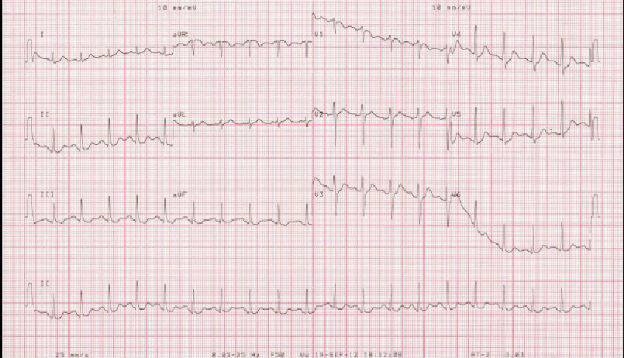
Figure 1B
-
1. How would you proceed: empirical radiofrequency ablation in the Koch's triangle, empirical cryoablation in the Koch's triangle, or no ablation and observe clinically?
Option 1: No ablation and observe clinically
ECG during palpitations showed SVT, which was compatible with AVNRT. However, only dual AV nodal physiology and single AV nodal echo beat were inducible. There will not be any reliable procedural endpoint. One may attempt empirical radiofrequency ablation and look for slow junctional beats during ablation, but the low but genuine risk of inadvertent AV block may not be justified in this case. One may also attempt empirical cryoablation and look for loss of slow pathway conduction.Catheter ablation was not attempted, and the patient was given flecainide on discharge. However, he was admitted one month afterward for fast palpitations, and ECG again showed SVT that required termination with intravenous adenosine.
Another cardiac electrophysiology study was performed. This time, no dual AV nodal physiology could be demonstrated and no AVNRT could be induced. Nonfluoroscopic three-dimensional images are shown in Figure 2A and B. A large ostium of coronary sinus with the bundle of His just at the superior margin of the ostium was revealed.
Option 2: Empirical cryoablation in the Koch's triangle
The patient had recurrent SVT with ECG compatible with AVNRT. The arrhythmia was also refractory to both verapamil and flecainide. Unfortunately, the arrhythmia has been difficult to induce in the electrophysiology laboratory. Withholding ablation the second time is acceptable but not optimal in this situation. The unfavorable anatomy in the Koch's triangle speaks very much against the choice of radiofrequency as the source of energy for empirical ablation. Empirical cryoablation in this case strikes the best balance between safety and clinical effectiveness.Empirical cryoablation was performed with a catheter with a 6 mm tip. Multiple lesions were placed near the region of the bundle of His (Figure 2 A and B). Cryomapping at a temperature of -30°C was performed to guarantee the absence of inadvertent AV block before cryoablation. Flecainide was stopped after the ablation, and the patient has been free of recurrence of SVT for 6 months after ablation.

Figure 2A

Figure 2B