The Practice of Catheter Cryoablation for Cardiac Arrhythmias
Edited by Ngai-Yin Chan


Cases
Case 5.1. Cryoballoon Pulmonary Vein Isolation for Atrial Fibrillation
A 78-year-old man presented with a several year history of irregular rhythms which were incessant and unresponsive to beta blockers, calcium channel antagonists, and Class Ic antiarrhythmic agents. Documented arrhythmias included atrial runs, fast regular and irregular supraventricular tachycardias, and atrial fibrillation.
The patient complained of shortness of breath, lightheadedness, and syncopy. Coronary artery disease was ruled out by coronary angiography.
The resting ECG showed atrial runs and irregularly conducted atrial tachycardias (Fig. 1). Further analysis revealed a shifting morphology of the focal P waves with an unchanging inferior axis and biphasic P waves in lead I, a negative P in avL and the P wave becoming positive and notched in V1.
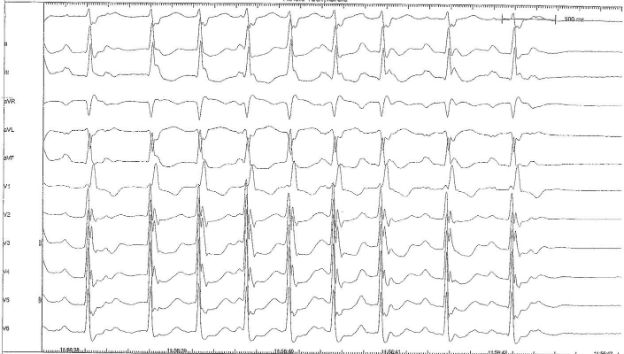
Fig. 1: Focal Atrial Tachycardia
-
1. Which is the most adequate clinical approach?
-
2. During focal activity, the typical reversal of pulmonary vein spikes and atrial far field was observed in the right upper pulmonary vein. The same type of phenomenon was seen when the Achieve catheter was used, which provided the same quality data (Fig. 2). What is the diagnosis?
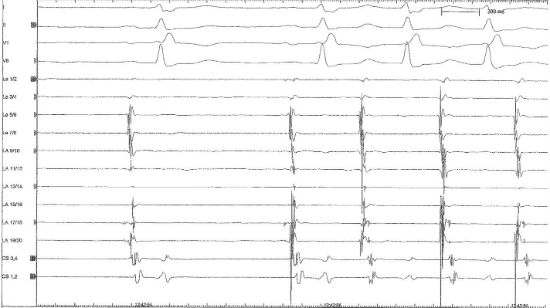
Fig. 2: Lasso RUPV
-
3. Describe the next steps in treatment
Correct answer:
Treatment: Under continuous phrenic nerve monitoring, right upper pulmonary vein isolation was completed with two freezes using a 28mm balloon. The incessant focal activity came to a complete stop during the 1st freeze. The surface ECG demonstrated a regular rhythm (Fig. 3). Because of the possibility of crosstalk between the ipsiseptal veins, the right lower pulmonary vein was also isolated with two freezes.
Now, six months after the intervention, the patient remains free from arrhythmias.
Fig. 3: ECG after first Freeze of RUPV