The Practice of Catheter Cryoablation for Cardiac Arrhythmias
Edited by Ngai-Yin Chan


Cases
Case 8.2. Catheter cryoablation for the treatment of accessory pathways
A 62-year-old woman presented with recurrent paroxysmal palpitations for 10 years. Electrocardiogram documented supraventricular tachycardia (SVT). She was given Sotalol with refractory symptoms. A cardiac electrophysiology study revealed a concealed paraHisian accessory pathway with inducible orthodromic atrioventricular reciprocating tachycardia (Figure 1).

Figure 1
-
1. What would be the appropriate ablation strategy – radiofrequency ablation with a 4 mm tip catheter, cryoablation with a 4 mm tip catheter, cryoablation with a 6 mm tip catheter, or cryoablation with an 8 mm tip catheter?
-
2. What should be the criteria for successful cryomapping – termination of SVT, absence of inadvertent atrioventricular block, and/or loss of concealed paraHisian accessory pathway conduction, or all of the above?
Correct answer: Both termination of SVT and loss of concealed paraHisian accessory pathway conduction are evidence for appropriate target site. However, termination of SVT can be a nonspecific response to catheter manipulation. Loss of concealed paraHisian accessory pathway conduction during ventricular pacing remains the confirmatory endpoint for effective cryomapping. Apart from assessment of the effectiveness of cryoablation at the potential target site by cryomapping, it is even more important to look for risk of inadvertent atrioventricular block.
Cryomapping resulted in ventriculo-atrial dissociation, failure to induce SVT, and absence of inadvertent atrioventricular block (Figure 2). A permanent lesion was then delivered to the same site by lowering the temperature of the catheter tip to -75°C.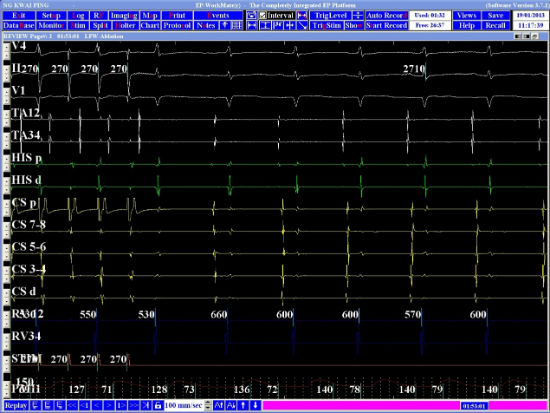
Figure 2